
If you don’t do good chest compressions, you’ll enjoy a great career in PM&R!
-One of my attending physicians
*As in all my posts, patient details have been changed for anonymity, but the core story is true
This line comes from my favorite story from medical school, which I’m going to tell shortly. While I enjoy my standard format of tell a story -> relate that story to a concept -> expand and/or educate on that concept, I want to be very clear what this post is about:
There is going to come a time in your life where someone you love (or quite possibly you) is Sick. I mean Sick with a capital “S”: the kind of sick that results in the only certainty in life besides taxes and that new admissions will always come in 1 minute before changeover: death. Until we can preserve a person’s head in a jar and keep them alive forever Futurama-style, everyone that is born is also going to die. While some people will die in a fantastic, gruesome fashion like doing a pile of cocaine in a pile of strippers, most of us will die in a protracted course from a chronic disease. We might not have a lot of control over what eventually kills us, but we can have a big say in the way we die.
The medical community is in the midst of a significant paradigm shift when it comes to how we think about death, so allow me to share these thoughts with the medical and non-medical folks alike. Specifically, this post is about the time when you’re going to have to make a decision about taking care of your parents, siblings, or grandparents when they are nearing the “DC to JC” as one of my attendings calls it: the discharge to Jesus Christ. You will be involved in the decision of how we, as physicians, should treat your loved one at the end of their life. This can include questions such as, “Do we continue treating their stage IV cancer?” and “Do we want to put grandpa on dialysis for his failing kidneys when he can’t even wake up?” There are a multitude of things to consider when feces hits the fan, but it boils down to this basic question:
“Do we want to keep doing everything we can to keep our loved one alive, or do we want to make them comfortable as they are dying?”
The example I’m going to use to explain all of this is called code status. Code status on a patient mainly refers to one of three states: full code, partial code (most likely no CPR or no intubation), or DNR (do not resuscitate). This is something patients should be asked when they enter the hospital as to what their wishes were if they were to “code” – meaning in laymen’s terms that their “heart has stopped”. This is a decision you will likely make for someone else someday, and a decision you should make for yourself too. I’m going to go into why often times prolonging someone’s life isn’t the right answer, especially in certain situations; also, I’ll explain why quality of life and a dignified death should be the main goal in end of life care. Now, back to the story…
–
“Code blue, day surgery“. My intern and I froze, as everyone in the hospital did for that moment. The calm, female voice echoed throughout the hospital. Code blue means that either a patient’s heart or lungs are in trouble. It could be that a patient’s heart is either not pumping at all or is sitting there quivering, unable to generate the force it needs to pump blood to the rest of the body. Whereas a normal person’s heart generally beats anywhere from 60-100 times per minute, a code blue due to a heart issue means that person has a functional heart rate of 0. Normal people breathe 12-20 times per minute; a patient in a code blue could be breathing much faster or much slower than normal, unable to sustain their breathing. Code blue means they need doctors, nurses, therapists, and more to come rushing to their aid. Code blue means someone is dying.
After that brief, heart-stopping instance, we breathed a sigh of relief. There was no way that was one of our patients. We didn’t have anyone in day surgery at that time. If we did, the scene would have been much different, as we would have sprinted to day surgery to help fix whatever disaster was emerging. Instead, we simply went about our duties, because by that time there would be dozens of people at the bedside. We went on to see our next patient, asked them if they had pooped that day (probably the most common question that surgeons ask, I never thought poop would one day run my life), and moved on to the next task. Announcements of a code are fairly frequent in a hospital. Therefore, for us, today would continue just like any other day.
Except today wouldn’t continue just like any other day. That patient coding was our patient. A patient that we had operated on only 2 hours ago. This would be my first code.
We walked back up (just kidding, we took the elevator. Stairs are hard) to our team room some 15 minutes later, when someone from the other surgery team we shared our room with said, “Yo, do you guys know anything about that guy coding down in day surgery? He just had a rubber duck transplant.” It felt like I had stepped into a vacuum, the air gone from the room around me. We just did a rubber duck transplant (surgery obviously changed for anonymity) on a guy who fit that description. That was our patient. My intern registered this before I did, and had already ran out the door by the time I had regained my state of mind to follow him. The sprint and elevator ride down to day surgery was filled with alternating periods of profanities and silence. Our patient was relatively young, our patient was here for a simple outpatient surgery, and our patient had pretty much no comorbidities (conditions such as diabetes, heart disease, or many other things that make them more “sick” and likely to have bad outcomes such as a code). This just didn’t fit.
The scene that greeted us was organized chaos, like all codes are. By this time, several months into my 3rd year of medical school, I had seen a code or two, but had never participated in one, let alone on my own patient. It felt…different. The room was packed, with a crowd of around 30 people crammed both in and outside of the room. There were plastic wrappers and trash littering the floor and people power-walking in and out of the room with another piece of equipment in hand. I could see the back of my attending physician’s head from where we stood. A burly guy, sweating from exertion, walked out of the room as we arrived and said, “We need help on the chest!” By that time, the code had been going for 15 minutes, and they needed other people to help rotate through doing chest compressions. We threw our white coats to the side, put on gloves, and stepped into the fray.
The bed was high off the ground, our patient sprawled on top. An ICU attending was at the back of the room yelling out orders. An anesthesiologist and resident stood at the head, controlling the patient’s airway. A female resident, standing somewhere in the neighborhood of 5’0″ and 100 pounds soaking wet, was perched high on a stool delivering forceful blows to the patient’s chest. An array of nurses were helping obtain supplies, a resident was frantically trying to put in a femoral arterial line, and a pharmacist was out medications from the code cart. We stepped in line for compressions, as it had dwindled thin with time.
As I stood there, I recalled the line from possibly the greatest medical book of all time, The House of God, “The first step in a code is to take your own pulse“. I remember moving my fingers to my radial artery, closing my eyes, and drawing in a long, deep breath. I took those few seconds to compose myself and took my heart rate. 80. Not normal for me at rest, but I could work with it. “SWITCH!” got called out, and the person in front of me stepped up to the chest. A brief break was called to check pulses. “NO PULSE! RESUME COMPRESSIONS!” The guy in front of me thumped away. This is where what you see in medical shows isn’t too far from the truth when it comes to a code. The only difference is that there are usually three times as many people in the room, as well as in TV they have TERRIBLE form when it comes to chest compressions.
–
I stared at the rhythm strip on the small screen from across the room. The heart monitor or defibrillator measures the electrical activity of the heart, and that’s what you see when you hear the “beep…beep…beep” along with the little squiggle that represents how voltage flows through the heart. When someone’s “heart stops”, it generally means their heart is in one of four possible rhythms. Asystole is the “flatline” that you frequently see on TV and in movies. This is when the heart is not only not pumping, but has no electrical activity either. This is bad, and in real life you can’t shock this rhythm with a defibrillator. All we do is chest compressions, push a few drugs, try to fix the underlying cause of their heart problem, and pray to the code gods that their heart restarts. The other of the non-shockable rhythms is called pulseless electrical activity, or PEA. This is exactly how it sounds: the heart has electrical activity but isn’t pumping.
Shockable rhythms include ventricular tachycardia and ventricular fibrillation, the former is when the heart is beating so fast that it isn’t effectively pumping blood, thus also causing a lack of blood flow. It has the danger of devolving into the latter: when the heart is “quivering” and not pumping sufficiently, but still has electrical activity. For these, we do the same things as the non-shockable rhythms except we add, you know….shocking them. Yes, we really yell “CLEAR!” Yes, the patient briefly jumps off the table due to muscle contractions. And yes, it sometimes actually works. The point I’m trying to make here is that shocking someone isn’t always the answer in a code. We check the so called “H’s and T’s” for the reversible causes of cardiac arrest. Something like high or low potassium, a massive blood clot in the lungs, low oxygen levels, or massive blood loss can cause cardiac arrest; these things can be fixed and often return the heart to working order. Alright, learnin’ is done here, back to the story.
–
After another two minutes of compressions, it was time for me to move from my “on-deck” status to step up to the plate. I stepped up on the stool (who would have ever thought a lanky 6’3″ guy would need a step stool?! I was a little flustered based on that alone. I guess my tall ego had a long way to fall to the floor. Turns out the bed was actually about a foot higher than it needed to be for some insane reason. Step 1 in a cardiac arrest is lower the bed as low as possible, step 0 being call for help) and assumed the position. “RESUME COMPRESSIONS!” It took me all of 5 seconds to figure out just how tiring chest compressions were. This guy had a BIG chest, so maybe that played a part, but turns out it takes a lot of force to compress someone’s rib cage hard enough to pump their heart. The song “Staying Alive” by Bees Gees is at approximately the rate of chest compressions, 100bpm, so I remembered singing that song in my head. Also the mantra of “press hard and fast, at least 2 inches, and let the chest recoil, repeat” kept echoing through my brain. (Which reminds me of this classic flash video of the Metal Gear Solid Crab Battle. Counterbalance the knife, quick stab, retract.) However, my somehow out-of-tune singing in my head was quickly drowned out by the activity of the room. The gravity of what I was doing at the time didn’t quite hit me. I was fighting for this patient’s life with my own hands. Without these compressions, he would experience profound hypoxic injury very quickly. It was at this point, some 30 seconds into my round of compressions, that my attending drops this gem:
“If you don’t do good compressions, you’ll enjoy a great career in PM&R!”
The entire room erupted in half-nervous, half-genuine laughter. The entire scene was ridiculous. Here I was, my first time doing chest compressions on a human being, on a patient I helped operate on no less, trying my best to slam blood throughout his body, and my attending was roasting me in front of a room of 30+ people. Hardly an ideal time to crack a joke, but sometimes the most morbid of times are when they are most needed. For those of you that don’t get it, my attending was a surgeon and knew I wanted to go into surgery. PM&R stands for Physical Medicine and Rehabilitation, a specialty that is about as far from surgery as it gets. He was making a joke that I wouldn’t make it as a surgeon otherwise. It took everything I could to not bust out laughing, because as harsh as that quote might sound, he’s the kind of person who makes sarcastic jokes all the time. If he’s making fun of you, he likes you, and if he doesn’t speak to you, you should worry. To put this in context, he once cracked a joke as our team was eating that I “Did a sh*tty job!” taking out a gallbladder in a surgery with him, and that was the greatest compliment I’d ever received in medical school. It’s his form of praise. Surgeons are weird.
So here I was, a room full of people laughing in an attempt to take our minds off of what was happening in front of our eyes: a patient was dying (technically dead with a heard rate of 0) with little hope of revival. It had already been between 25-30 minutes of “code time” by this point, a threshold past which people usually don’t survive. The longer a code goes, the worse the prognosis is. Even if they survive, they often have a profound injury (usually brain) from the lack of oxygen to the tissues. In hindsight, my attending was also attempting to lighten up the situation for himself, as he was watching one of his patients die. “SWITCH, PULSE CHECK!” I stepped down from the stool, panting, and got back in line. Who needs barbells when you have hearts to pump?
The cycle kept repeating in 2 minute intervals. The ICU attending was having a conversation with the other physicians and nurses about what else to try, what new labs we had gotten, and looking for a cause. Codes are a team effort, there is more than one person doing all the thinking. Our minds don’t work very well under high stress (except in those who have practiced, and I’d say most doctors get a fair amount of practice), and it often takes a room full of people operating at near-braindead status to think clearly. Suddenly, after I stepped off the stool for the nth time and they shocked him, our patient got a perfusing rhythm. Huzzah! That means we could feel a pulse and his heart was beating on its own. He has been through both PEA and ventricular fibrillation and he somehow got his rhythm back. However, that lasted only 30 seconds and…back into Ventricular fibrillation. Thus, the cycle continued. The question popping up was…when would we stop?
See, in a code, the decision to stop is made by the physician in charge (and by extension the team as a whole). There isn’t some proven, scientific way to say when a code should end. Like a lot of things in medicine, it is an art: a combination of clinical knowledge, intuition, experience, and critical thinking all rolled into one. In this case, it was a relatively healthy patient who was fairly young (by hospital standards, this means <60 years old), and we were going to keep trying. In a very sick, frail man, we might have stopped long ago if he wasn’t getting any signs of a perfusing rhythm.
In this case, the lead physician (the ICU attending) wanted to plow ahead. We spent another 20 minutes with our patient flickering in and out of perfusing rhythms, sometimes for seconds, sometimes for a minute or two. Finally, we managed to establish a perfusing rhythm for a few minutes! He even tried to jump off the bed as he woke up, all Frankenstein-style, and was promptly sedated for his (and our) safety. My entire torso was burning by that point, but by golly we had done it. They whisked off the patient to the cardiac unit. As the room emptied, I took a moment to take in my surroundings. The room was a mess, a graveyard of discarded medical packaging, with even a full central line kit laying unopened on the ground. There was blood dotting the floor and the wall. There were other sweaty people who had finished doing compressions. I could feel the waves of adrenaline (norepinephrine) receding and felt the crash coming. What? Just? Happened? It was a blur, and recalling this many months later, I can’t remember all the details. I don’t think I could have remembered them any better even if it was the day after. My intern and I looked at each other, grabbed our white coats from the nursing station, slid them on, and walked off to resume business as usual. Not a word was spoken. We went from sheer chaos right back to our next task. The world rotated on, the heart monitors kept beeping, and there was another patient to see who hadn’t pooped in 4 days.
–
The scene I described is pretty textbook for how it happens in the movies and in TV shows: the heroic doctors come to a bad situation with a dying patient, turn it around, and they end up being completely fine with no long-term complications. The patient is typically young, has a random cardiac arrest, and gets brought almost instantly back to life. You’re probably not going to be surprised when I tell you that isn’t at all like real life.
Fact of the matter is, most patients who code do not survive. The American Heart Association puts out some statistics on this, and in 2016 the survival rate for out of hospital cardiac arrests was 12% and in-hospital was 24.8% (I didn’t read the entire report, but the parts I did read were fascinating). Now, those survival rates mean survival to hospital discharge, meaning that it is likely that many of these people survive initially only to die in the hospital, probably from sequelae of their arrest. A search on UpToDate (a website that aggregates current research in medicine to provide an easy way for physicians to practice the most current evidence-based medicine) supports this conclusion, indicating that in one study for patients with Pulseless Electrical Activity (PEA), 23% survived to hospital admission and 11% survived until discharge. The UpToDate article is called “Prognosis and outcomes following sudden cardiac arrest in adults”. In asystole, about 10% of patients with out-of-hospital arrests survive until hospital admission, with between 0-2% surviving until discharge. While the survival for ventricular arrhythmias is much higher, where somewhere between 25-40% survive until discharge, this means the overall survival chances are still very grim.
And even in those that survive, there is a high incidence of permanent damage. Again according to UpToDate, in one study of patients who had Vfib arrest out of hospital, only 40% had “mild or absent neurologic impairment on discharge”. Folks, that means 60% had some degree of moderate or severe neurologic impairment, despite surviving. And that’s only one study, I decided to not include more so as to make this not full of studies and data, as that isn’t the point of this post. It turns out organs like your brain enjoy having oxygen. Even when someone’s heart is being pumped for them, they don’t always get the oxygen they need. Either that or their respiratory drive shuts down, they can’t get off the ventilator and support their own breathing, they experience kidney failure from lack of blood flow, or one of a thousand other things that spell a r-e-a-l-l-y t-e-r-r-i-b-l-e o-u-t-c-o-m-e. A cardiac arrest is a huge insult to the rest of the body, and then getting thumped on (which, by the way, usually breaks multiple ribs) and pushed full of drugs doesn’t exactly help.
The point here is this: even after initially “surviving” a cardiac arrest, a patient is very likely to not have a meaningful recovery. This means some patients get put on ventilators and never come off, they never become fully conscious again, have severe neurologic problems (like not being able to talk), or any number of things. The more sick that someone is beforehand, the less likely they will recover from such an event. Therefore being more sick (known as having multiple comorbidities) and chance of survival from cardiac arrest are then “inversely proportional”. Bet you didn’t think you’d see that elementary school math term come out again.
“But wait!” some people might say, “grandma was doing just fine before she had a heart attack that caused cardiac arrest!” There’s an important concept I want to explain here: physiologic reserve. Think of someone’s health like a large, gradual, sloping hill that goes down and down at a fairly easy angle. The angle gets a little steeper the further you go down, but not by much. At the end of the hill, there’s a cliff that drops into a ravine the size of the Grand Canyon. The young, healthy 25 year-old sits high atop that hill. The might get an illness like a cold, the flu, or even something more severe like pneumonia, that will push them closer towards the cliff. But, since they are high up on the hill to begin with, they only go down a little ways towards the cliff. They have a lot of room to recover, which is represented by moving back up the hill. Let’s say they get something terrible like a heart attack that pushes them very far horizontally towards the cliff. Again, because they were so high to start with, that horizontal movement towards the cliff still leaves them able to recover because they have a lot of physiologic reserve. In this analogy, physiologic reserve is the distance they are from the cliff”. I’ve made a masterpiece of a paint image to illustrate this concept:
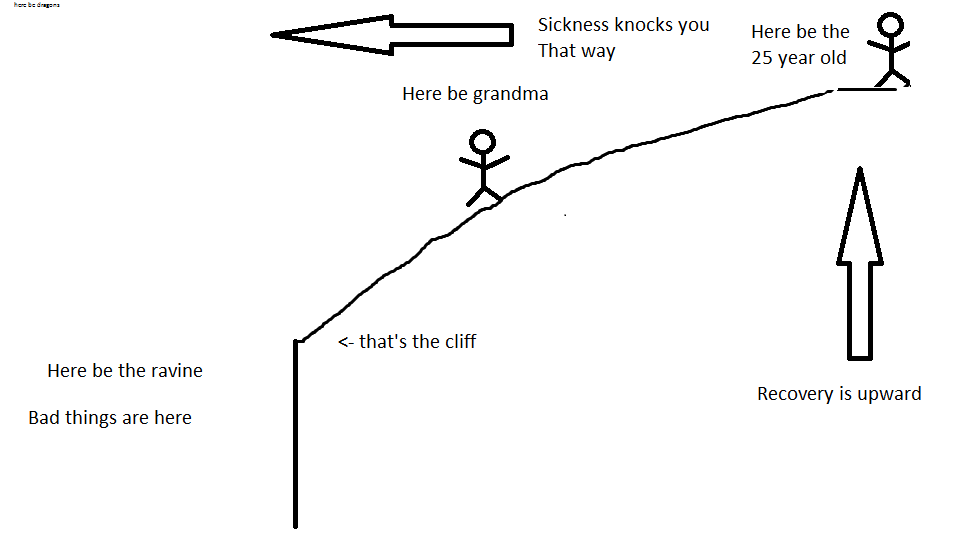
However, let’s take grandma. She’s older, maybe in her 70’s or even 80’s. She has emphysema or chronic obstructive pulmonary disease (COPD) because of smoking for 50 years, some coronary artery disease, and diabetes. She starts FAR down the hill from the 25 year old, not only because of her age, but also because of the other conditions she has. Her lungs don’t work as well as they should, she often has high blood sugar, and the arteries to her heart are a little clogged. This means that if she gets something like a cold, it knocks her the same horizontal distance down the hill. Since she is on the steeper part, it takes her longer to get back to where she was. She therefore falls more vertically than the 25 year-old, so her rehabilitation takes much longer. This also means she has less of a reserve – basically a buffer that is able to absorb being sick. However, if grandma gets something bad like pneumonia in both lungs or a heart attack, this has the ability to knock her so far down the hill she falls off the cliff. That cliff means might mean time in the intensive care unit, never being able to recover to her previous level of health, or death.
Those people who have less physiologic reserve, such as the elderly or the chronically ill, don’t deal very well with a hit to their health. This concept is what drives our discussions about end of life care with patients and their families; one of the most important is known as “code status”. Code status is a set of directives for what we (the doctors, nurses, etc.) should do if someone goes into cardiac arrest. It most commonly deals with two things: the options regarding mechanical ventilation, aka sticking a breathing tube down someone’s throat and putting them on a ventilator, and the option regarding CPR (cardiopulmonary resuscitation). The question is, “What do you want us to do to get your heart and lungs working again?” Turns out, this is an immensely important question.
Let’s do a few examples here. First up is your mother or father. Let’s say they’re 55, have high blood pressure and maybe a little pre-diabetes for good measure. Mom watches her blood sugar, takes her blood pressure medication every day, exercises, and is a little overweight with a BMI of 28. She gets admitted to the hospital because she got pneumonia from working at a nursing home. If I was her doctor, I’d explain how she’s in fairly good health and ask her what she would want her code status to be. If her heart were to stop, would she want us to put a breathing tube down her throat, do CPR, shock her, and do everything we can? I’d likely leave it at that. With otherwise healthy patients, we’d expect them to survive a code. Often with these patients, the talk about code status might only be a sentence or two long.
Second, let’s take grandma. She’s 70, has diabetes, high blood pressure, some COPD from smoking (although not using home oxygen), and pretty bad heart disease. in fact, she has had open heart surgery for clogged heart arteries. She’s fairly sick, and we might want to be able to put a breathing tube down here throat, called intubation, if she wasn’t able to breathe well. However, if she were to have a heart attack or something that would stop her heart from beating, we might recommend to not do chest compressions or shock her because her heart isn’t likely to recover. This is because she doesn’t have much physiologic reserve in the first place. For someone like this, the discussion about code status would be a little longer. We might push towards allowing intubation but not CPR, which would make her a “partial code”.
Here’s the last example: this time it’s your uncle. He’s 48 ans has been an alcoholic his whole life. He has significant liver damage, has turned yellow (jaundiced) because of liver failure, has fluid in his belly (ascites) due to the high blood pressure in the veins to the liver, and has dementia due to buildup of toxins a healthy liver would filter out (hepatic encephalopathy). He is still drinking, and therefore not a candidate for a liver transplant. When he comes into the hospital because of infection in his belly fluid (spontaneous bacterial peritonitis), I would sit down and have a long talk with him, if he is lucid, and his family if he is not. The main point is that not only is his life expectancy probably very short (he could have as high as a 50% chance of dying within 3 months), but he would be unlikely to survive cardiac arrest, let alone recover from one. For him, we would recommend him being DNR/DNI. This stands for Do Not Resuscitate/Do Not Intubate. This means if his heart stops, we would make him comfortable with pain medicine and let him die peacefully, rather than with 30 people slamming on his chest, breaking ribs, and shoving lines and tubes into him.
This point is the same for your 90 year old grandmother, your 75 year old grandfather with Stage IV (the worst stage) colon cancer, or your brother who got shot in the head and will never recover: making your sick family member DNR (also known as no-code) will let them die peacefully. The alternative is putting them on a ventilator, breaking nearly all of their ribs, and probably dying in the intensive care unit hooked up to every machine known to modern medicine. Death is one of the most complex, most difficult, and most emotionally charged concepts that we deal with as physicians; you will deal with it as a friend, family member, or patient. It is a muddled sea of grey, where there are no right answers and few certainties. We can speak in probabilities, prior experience, and clinical knowledge, but cannot predict the future. That being said, there are ways in which we can both make sure people experience the least suffering and die without undergoing unnecessary (and painful) treatment.
The overarching theme is how we go about managing the care of people at the end of their life. In this world of life-prolonging complex medical procedures and interventions, the question is not can we do them, but should we do them? Such a question begs an entire post devoted to the subject. However, you and I should keep that question in the back of our minds when it comes to discussing code status. The focus in medicine has been shifted away from keeping patients alive at all costs towards preserving quality of life, even at the expense of shortening time spent alive. Dying isn’t the worst possible outcome. I’d argue dying of multiple organ failure after spending a week on a ventilator is.
When it comes time for you to make medical decisions for your loved one, please consider the overall outlook. Dying at home, comfortable, with friends and family around is a dignified death. A happy death. A comfortable death. Consider making your loved one DNR if appropriate, and consider their quality of life going forward. Think about what you would want if you were being kept alive only because of a ventilator. Have these discussions with your siblings, family members, and friends early; you don’t want to have to try to read someone’s mind when they’re already critically ill. When a doctor comes to have that discussion with you, be open to considering that “doing everything” isn’t always the right thing.
Oh, are you wondering what happened to my patient from earlier? He walked out of the hospital two weeks later. I must have done some damn good compressions.
-Brandon
Today’s music is from probably my favorite duo Timeflies and their cover/sample of Someone Like You
